
An insulin pump is one of the most advanced methods of diabetes management, especially in children with type 1 diabetes. In this method, insulin is delivered continuously and on a schedule to mimic the natural function of the pancreas. To better understand the pump settings, we need to understand two main concepts: Basal and Bolus.
How does an insulin pump work?
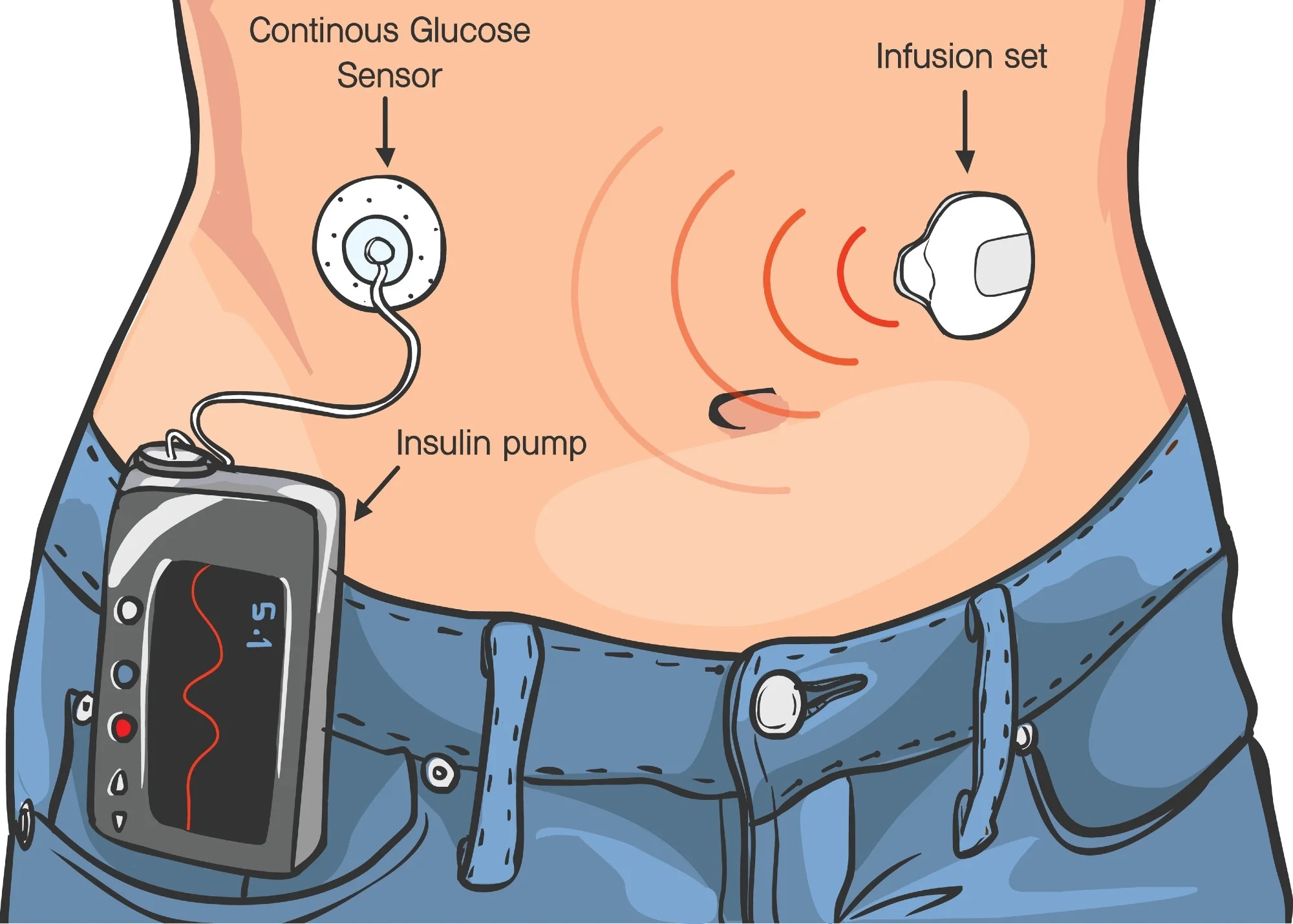
A pump is a small device that injects fast-acting insulin through a thin tube (infusion set) under the skin. Unlike daily injections, this device intelligently adjusts the amount of insulin throughout the day.
What is Basal? (Basal Insulin)
Basal means a small amount of insulin that is continuously delivered throughout the day, even when the child is not eating.
Why is Basal important?
Our body needs insulin even when fasting to:
Keep blood sugar stable
Prevent the liver from producing too much sugar
Features of Basal in children:
In children, the need for insulin varies at different times of the day
For example:
Early morning (dawn phenomenon): higher need
Midnight: lower need
Basal setting:
Your doctor or treatment team usually sets Basal on an hourly basis. This means that the pump may deliver a different amount of insulin each hour.
Simple example:
00:00 to 03:00 → 0.3 units per hour
03:00 to 07:00 → 0.5 units per hour
07:00 to 12:00 → 0.4 units per hour
These settings are completely personal and are based on:
Child’s age
Weight
Activity level
Sleep pattern
And blood sugar results
What is a Bolus? (Meal insulin)
Bolus is the amount of insulin injected to eat or correct high blood sugar.
There are two main types of bolus:
1. Meal Bolus
When the child eats food, blood sugar rises. To control this increase, a bolus is given before or during the meal.
How is it calculated?
Using an important ratio called:
Carbohydrate to Insulin Ratio (ICR)
That is:
How many grams of carbohydrate are covered by 1 unit of insulin
Example:
If ICR = 1:15
That is:
Every 15 grams of carbohydrate → 1 unit of insulin
If the child eats 45 grams of carbohydrate:
→ 3 units of insulin are needed
2. Correction Bolus
If the child’s blood sugar is above the target level, this type of bolus is used to lower it.
Based on what?
A factor called:
Insulin Sensitivity Factor (ISF)
Means:
Every 1 unit of insulin lowers blood sugar by how many mg/dL
Example:
ISF = 50
Means:
1 unit of insulin → lowers blood sugar by 50 units
If blood sugar:
Current: 200
Target: 100
Difference = 100
→ need 2 units of correction insulin
Other important settings on the pump
Active Insulin Time
The length of time that insulin is active in the body (usually 3 to 5 hours). This setting helps prevent over-injection.
Advanced Bolus Types
There are different types of Bolus in pumps:
Normal Bolus
For simple foods like bread or rice
Square Wave Bolus
For fatty or protein foods (like pizza) that raise blood sugar slowly
Dual Wave Bolus
A combination of fast + gradual
Suitable for mixed meals
Important points in children
1. Greater sensitivity to insulin
Children (especially young children) may experience hypoglycemia with low insulin doses.
2. Variable physical activity
Playing and moving a lot cause blood sugar to drop → Basal or Bolus may need to be reduced.
3. Growth and hormones
During growth:
Insulin needs change
Settings should be reviewed regularly
4. Role of parents
Parents should:
Learn to count carbohydrates
Check blood sugar regularly
Coordinate settings with doctor
What is the purpose of proper settings?
Prevent low blood sugar (hypoglycemia)
Prevent high blood sugar (hyperglycemia)
Improve the child’s quality of life
Reduce long-term complications
A simple example of a real day
Let’s assume the child:
Breakfast: 30 grams of carbohydrates
ICR: 1:10
→ Meal Bolus: 3 units
If pre-meal sugar:
180 (target 120)
ISF: 60
→ Correction: 1 unit
Total Bolus: 4 units
In addition, the pump automatically delivers Basal throughout the day.
Simple summary
| Type of insulin | Role |
|---|---|
| Basal | Controls fasting blood sugar |
| Bolus Meal | Controls post-meal blood sugar |
| Correction Bolus | Lowers high blood sugar |
How to set Basal accurately?
Setting Basal correctly is one of the most important and at the same time the most sensitive parts of working with the pump.
Basal Testing
To find out if Basal is set correctly or not, the “Basal Test” is used.
Simple method:
The child does not eat for a period of time and only blood sugar is checked.
Conditions for performing:
Blood sugar at the start of the test is within the target range
The child is not sick
No unusual activity
Example:
If we test from 12 to 4 pm:
Blood sugar is measured every 1–2 hours
Conclusion:
If blood sugar remains stable → Basal is appropriate
If sugar rises → Basal is low
If sugar falls → Basal is high
Basal classification in children
A child’s body does not have a fixed pattern, but some common patterns are seen:
Dawn Phenomenon
From 4 to 8 am:
Growth hormones and cortisol ↑
→ Blood sugar rises
→ Need for more Basal
Midnight
In some children:
Need for less insulin
→ There is a risk of hypoglycemia
Evenings
If the child is active:
Insulin sensitivity ↑
→ Basal may need to be reduced
Bolus adjustment More Professional
So far we have explained the general concept, now we will get more specific.
Real Challenges in Food Bolus
1. Mixed Foods
Like:
Pizza
Lasagna
Fatty Foods
These foods:
Raise sugar later and longer
Solution:
Use Dual Wave Bolus
Example:
50% Instant
50% in 2 hours
2. Fast-Absorbing Foods
Like:
Juice
Sweets
Need for Fast Bolus (Normal)
3. Mistakes in Carbohydrate Counting
This is one of the most common problems for parents.
Even an error of 10–15 grams of carbohydrates can:
Cause hyperglycemia or hypoglycemia
Fine-Tuning ISF and ICR
These two parameters should be adjusted regularly.
When do they need to be changed?
If:
Sugary always rises after meals → ICR is poor
We have frequent hypoglycemia → ICR is high
Or:
Sugary correction is not enough → ISF needs to be changed
Important concept: Insulin on Board (IOB)
Pumps have an important feature:
What does IOB mean?
It means:
The amount of insulin that is still active in the body
Why is it important?
If this amount is not taken into account:
→ There is a risk of overinjection and hypoglycemia
The pump automatically:
Calculates IOB
Includes a correction in the Bolus
Management of special conditions in children
Sick Day Management
When a child gets sick:
Stress hormones ↑
→ Blood sugar ↑
Measures:
Temporary Basal increase
Frequent glucose check
Ketone check
Exercise
Physical activity is one of the big challenges.
Effect:
Lowering blood sugar (sometimes severe)
Solutions:
Reducing basal before exercise (e.g. 20–50%)
Eating snacks
Reducing bolus before meal
Nights and sleep
Parents’ biggest concern:
Low blood sugar at night
Solution:
Adjusting basal at night accurately
Using a glucose sensor (CGM)
Setting alarms
The role of new technologies
CGM (Continuous Glucose Monitoring)
Sensors that:
Show blood sugar in real time
Identify trends
Smart pumps (Closed Loop)
Systems that:
Adjust basal themselves
They are also called “artificial pancreases”
The role of education in success
The important fact is:
The pump alone does not work miracles
Success depends on:
Parent education
The child’s understanding (at ages (above)
Collaboration with the treatment team
Common mistakes
Not readjusting as the child grows
Ignoring physical activity
Over-relying on the pump without checking blood sugar
Not giving a bolus on time
Making mistakes in counting carbohydrates
The ultimate goal
A good pump setting should:
Keep blood sugar in the target range
Reduce fluctuations
Make the child’s life more normal
Reduce parental stress
Advanced summary
The insulin pump acts like a “smart manager”:
Basal → background (like breathing)
Bolus → response to food and high sugar
IOB → prevent mistakes
Dynamic settings → adapt to the child’s life
Adjusting the pump in a child’s real life (practical scenarios)
Scenario 1: Breakfast and unruly morning sugars
Many children face this problem in the morning:
Blood sugar is normal before breakfast
But after breakfast it rises sharply
Why?
Insulin resistance in the morning (due to growth hormone)
Rapid absorption of carbohydrates (bread, honey, milk, cereals)
Professional solutions:
Bolus before meals (Pre-bolus)
10 to 20 minutes before eating
Strengthen the ICR ratio in the morning
For example:
Morning: 1:8
Lunch: 1:12
Morning Basal test
May need to be increased
Scenario 2: Normal lunch but high sugar afterwards
If:
Carbohydrate count is correct
But sugar rises 2–3 hours later
Probability:
Bolus is not enough or injected too late
Solution:
Careful ICR test
Use Pre-bolus
Pay attention to the type of food (fat? slow absorption?)
Scenario 3: Pizza and fatty foods
Common problem:
Normal sugar at first
A few hours later, it increases sharply
Why?
Fat causes:
Delayed gastric emptying
Slower carbohydrate absorption
Professional solution:
Use Dual Wave Bolus
Example:
40% immediate
60% over 3 hours
Scenario 4: Party and sweets
Challenge:
Child eats several times during the party
It becomes difficult to control
Solution:
Split Bolus into several parts
Use Correction Bolus if needed
More monitoring with sensor
Scenario 5: School
At school:
Unpredictable activity
Stress
Different foods
Important tips:
Set a more conservative Basal
Train a coach or teacher
Have an emergency plan
Temporary Settings
One of the most powerful pump tools:
Temporary Basal
That is:
Temporarily change Basal for a few hours
Applications:
Exercise
Decrease 20 to 50%
Start 1 hour earlier
Illness
Increase 10 to 30% (or (more depending on the situation)
Travel
Change in sleep/meal time
Need to reset
Understanding patterns (Pattern Management)
Pump adjustment is not just about giving numbers—it’s about analyzing patterns.
How to find a pattern?
Consider these questions:
Is the sugar high every morning?
Do we always have a drop after lunch?
Does the sugar drop at night?
Important rule:
A random number is not important, the “repeating pattern” is important
Example:
If 3 days in a row:
Lower sugar at 3 pm
You should:
Reduce the Basal for that hour
Or Reduce the Lunch Bolus
Step-by-step adjustment (Scientific Approach)
To avoid confusion:
The golden rule:
Only make small changes at a time
For example:
Change only the Basal
Or only the ICR
Not all at once!
Patience:
After each change:
Wait at least 2–3 days
Then draw conclusions
Important safety warnings
Risk of DKA (ketoacidosis)
In the pump:
Only fast-acting insulin is used
If the pump has a problem:
→ Insulin is stopped
→ Risk of DKA faster than traditional injections
Symptoms:
High sugar
Nausea
Vomiting
Rapid breathing
Urgent actions:
Check ketones
Inject insulin with a pen (if needed)
Replace pump set
Daily parent checklist
. Check blood sugar or CGM
. Check pump performance
. Check injection site
. Record meals and Bolus
. Pay attention to the child’s activity
. Check alarms
The psychological side of the story
We must not forget:
The child is not just a “patient”
He may get tired of the device
He may feel different at school
He may be upset by the restrictions
Role Parents:
Support without pressure
Gradual training
Giving the child a sense of control
The child’s future with an insulin pump
If the settings are correct:
The child can live a completely normal life
Exercise
Travel
Have a healthy growth
Final summary of this section
Pump management in children means combining:
Science (numbers and settings)
Art (understanding everyday situations)
Experience (learning from patterns)